Even very young women get uterine fibroids
Even very young women get uterine fibroids!
Written by Dr Karen Morton, Consultant gynaecologist and Founder of Dr Morton’s – the medical helpline - which has a special emphasis
on women's health and Dr Sarah Evans, Registrar in gynaecology at the Royal Surrey County Hospital, Guildford
I am not infrequently referred teenage girls, sometimes as young as 13 years, with dreadfully heavy periods, sometimes to the point of severe anaemia. There is usually no specific cause to find, but the following youngster’s story shows that they should be investigated thoroughly as rare things do happen……albeit rarely!
Sarah was 13 years old when her mother took her to her GP because she had fainted at school. She had been feeling exhausted for a long time but her mother took it as simply being a typical teenager; lying in bed until lunchtime over the weekend and being rather uncommunicative. Her periods had been heavy since they started at the age of 12. Her doctor gave her some tablets (tranexamic acid) to try to reduce the heaviness, and when after 6 months things did not improve she was started on a combined oral contraceptive pill.
One day about 6 months later, she started to bleed so heavily that she and her parents were really frightened and so they came to the accident and emergency department. On arrival, the bleeding was heavy with clots, soaking pads every 30 minutes. It was associated with lower abdominal pain. Sarah was sexually active, using condoms for protection. The bleeding was so heavy that it was at first thought this could be a miscarriage, but a pregnancy test was negative. Examination was largely normal, apart from looking very pale, with raised heart rate at 107 beats per minute and a mildly tender lower abdomen. A drip was put up and blood tests taken.
Sarah was very anaemic with a haemoglobin level of only 8.8 g/dl (it should be over 12) with a very iron deficient picture. Her blood iron level (ferritin) was unrecordably low. As this was such an unusual situation, studies were done to look for rare blood clotting disorders like factor VIII deficiency and Von Willebrand’s disease, but these were normal.
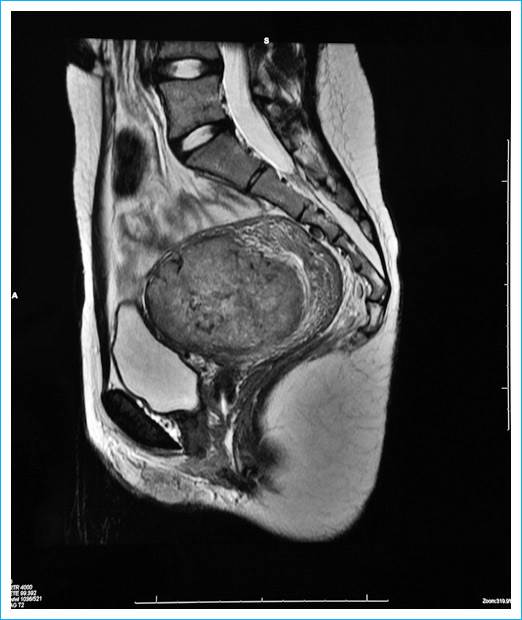
The next investigation was a transvaginal USS (TVUSS) which showed an enlarged uterus, with a large heterogeneous structure positioned centrally within the fundus measuring 6.5x5.3x4.9cm, suggestive of either a single large fibroid or three fibroids amalgamated. An MRI was sought to further define the fibroid, showed a vascular fibroid, situated interstitially in the anterior fundus and body of the uterus with a maximum dimension of 7.7 cm. It extended from the endometrium to the serosal surface of the uterus, in other words, very importantly, it occupied the full thickness of the uterine wall.
In view of Sarah’s youth, we tried to manage with more tranexamic acid at first, but as the bleeding continued to be dreadfully heavy, we had to do something else. Hysteroscopic myomectomy (chipping away the fibroid using a telescope inside the uterus inserted through the cervix) was not appropriate due to the fibroid extending through the full thickness of the uterine wall. It would have left a huge hole and would run the risk of damaging the bowel. Laparoscopic myomectomy was also considered but would have had the same overall effect of leaving a huge defect in the wall of the uterus. Although I had never considered uterine artery embolization (UAE) in someone so young, it seemed the best option. Consideration was given to the short length of hospital stay, reduced complications rate and reduced risk of reoccurrence with UAE, and in particular, the best chance of preserving fertility. This was performed without complication in December 2010, with Sarah was just 16.
Sarah was not the best attender for follow-up so when we did see her 3 years later we were thrilled to find her well, with normal regular periods and a TVUSS scan at demonstrated an almost normal looking uterus, with fibroid dead and calcified, measuring just 4.5cm and no new fibroids.
Uterine fibroids are extremely common in women of reproductive ages but much less so in adolescent women. This case explores the management of a young girl of 16, with heavy periods causing severe anaemia, and it shows that although very rare, significant fibroids should be considered as the underlying cause of menorrhagia in youngsters.
The management of fibroids in women who wish to retain fertility options is a controversial subject with limited data available to provide guidance. We are fortunate to be able to offer uterine artery embolization to our patients in Guildford. It is an evolving technique with ever increasing long term data showing good outcomes in terms of symptom resolution and comparable pregnancy outcomes to other methods of surgical intervention.
We believe this is the youngest case of elective uterine artery embolization recorded.
We are pleased to report that as of October 2018 Sarah now has a healthy 18 month old baby.